The dental papilla is the 3 dimensional soft tissue feature that is influenced by the following:
1-underlying alveolar morphology in relation to the contact point (Tarnow, Chu and Palmer propose that a distance of 5-6mm is highly predictive of papilla presence)
2-inter-radicular proximity
3-root circumference
4-tissue biotype
​As a periodontist, I can strongly affirm that restorative dentistry procedures cannot develop or produce dental papillae. If the above criteria are present then the papillae are usually present with sufficient patience ie. It can take time to develop particularly after implant placement or crown lengthening surgery.
Careful restorative procedures to develop papilla in my opinion only serve two roles:
- prevent trauma to the soft tissues therefore avoiding the cycle of loss and regeneration
- allow enough space for the soft tissues to form eg. Contact point length control to leave 5-6mm from the interproximal crest. If less than this distance is left then a flat papilla shape will develop.
So the million dollar question is: How do we regenerate papillae????
Consider optimising points 1-4 above depending on indications within the overall patient journey. I would definitely not consider interproximal grafting due to the poor blood supply in the interproximal space. We do not know factor is most influential in papilla regeneration and as such keep an open mind and always have a plan B!
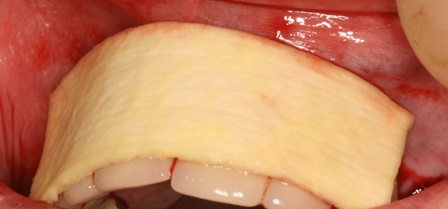
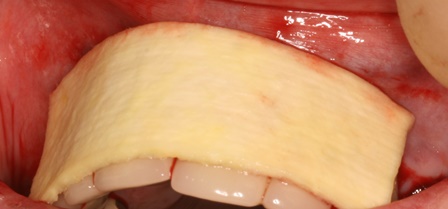
The case demonstrated is a simple example of altering tissue biotype with acellular dermal matrix graft to reduce recession on UR1 and to encourage the illusion of papilla around the pontics. This is a stable 6 month result. The resulting increase in the tissue biotype will facilitate easier closure during future bone augmentation if bridge fails. An alternative to this would be bridge removal and implant placement with ridge lap pontics which my patient wanted to delay for obvious reasons.
The use of soft tissue grafts to reduce recession has been shown to increase papillae height even in Miller Class 3 cases (Demirel et al 2015). This case is in keeping with the findings research reported in the scientific literature and discussed at the last Europerio 8 conference.