There are numerous clinical, logistic and financial advantages from linking teeth to implant restorations. Tarnow et al 2009 presented a literature review to on the subject of linking teeth and they sited a high risk of intrusion of abutment teeth in cases of parafunction or when semi-rigid (ie fixed movable) connectors were used. Palmer et al 2005 demonstrated high success rates with minimal critical complications like bone loss or tooth intrusion when linking teeth and implants with telescopic crowns and multi-unit bridge work cemented with temporary cement to allow for retrievability.
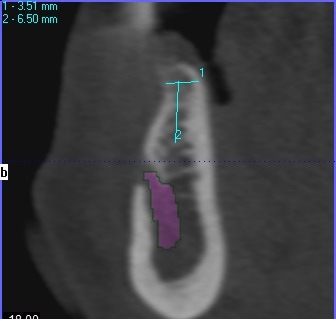
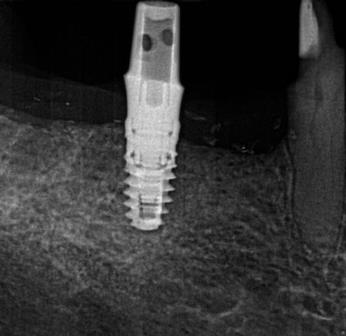
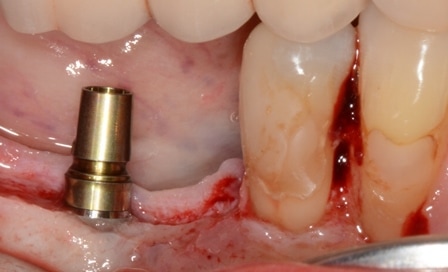
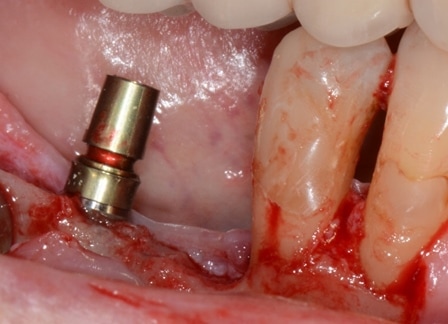
This approach was utilised for the presented patient to replace missing teeth in the posterior mandible which had extensive vertical and horizontal resorption. The resorption precluded placement of an implant in the LR5 region due to the proximity of the mental nerve and a concavity in the mental area of the mandible. Moreover, the LR4 was heavily restored in close proximity to the alveolar crest. This tooth would have an improved prognosis with crown lengthening and cuspal protection. It therefore became possible to consider placement of an implant in the LR6 position and to crown lengthen the LR4 at the same time. The eventual restorative plan would be to place a telescopic crown on the LR4 and a stock abutment on the LR6 implant and to link the two with a 3 unit bridge cemented with tempbond. This is in keeping with the Palmer et al proposed treatment journey.
The treatment plan was executed with ease and minimal morbidity. The alternatives include:
- placement of implant in the LR7 and LR6 to replace LR765 with a 3 unit bridge and to crown the LR4 separately. This would have increase costs biologically and financially and was rejected by the patient.
- implant in the LR6 along with removal of the LR4 to place an implant in its position, therefore allowing for a three unit prosthesis to replace LR456. This is highly complex due to the thin buccal bone in the LR4 site which will make placement of an implant in that site challenging. This option was rejected by the patient
- inferior alveolar nerve repositioning with implant placement in the Lr56 position for two separate crowns on the LR56. The high risk of paraesthesia makes this the least desirable alternative and as such the patient rejected it.
I would like to thank Juliette Reeves (RDH) for the exceptional post surgical maintenance and Paul Dumpleton (RDT) for the precise margins of the crown and bridge work.Â